On science blogs: Jolie laide
THE BREASTS OF ANGELINA JOLIE. I expected lots of blog posts about Angelina Jolie's double mastectomy. I didn't expect the torrent we're getting. My unscientific impression is that this is the single most-blogged-about medical topic I've looked at since I began writing On Science Blogs in 2009, going on 5 years ago.
Jolie knew it would be a big deal, of course, which is why, as Knight Science Journalism Tracker Paul Raeburn pointed out, she quite sensibly got out ahead of the story. If she hoped that would help her exert some control, she may be disappointed. I wonder if even she is surprised by the degree of clamor.

Perhaps it should have been predictable. Even in mad mediaworld this is an extraordinarily potent mix, involving a super-celebrity superstar who always makes news and sometimes scandal (and whose equally high-profile partner, here somewhat in the background, does ditto), plus women's breasts (two of them), plus breast reconstructive surgery, plus a cancer that is irrationally terrifying, and all of this soaked in a subtext of sex sex sex.
The fluff, with an occasional dollop of viciousness (especially on Twitter), is all-encompassing. I'm confining myself here to brief notes on a severely selected group of science and medical posts.
JOLIE'S PROPHYLACTIC DOUBLE MASTECTOMY: HER SURGEON SPEAKS. As part of her preemptive strike, Jolie gave her surgeon permission to describe her treatment. I suspect it was more than permission; it looks to me like PR orchestration, since doc Kristi Funk's post appeared on the same day as Jolie's New York Times op-ed revealing her surgery. It is of course matchless promotion for the surgeon and the outpatient clinic where it was performed, the one with the faintly mystical spa-ish name. This may be a most serious subject, but Hollywood is never far away.
Snarkiness aside, I thoroughly approve. Open case notes on a famous figure's medical condition are not unprecedented, but they are certainly unusual. It's a bit odd that so little has been said about these public details. The post is long and clinical, but not especially technical, and you would expect reporters and bloggers to have drawn upon it. So far as I can determine, few did.
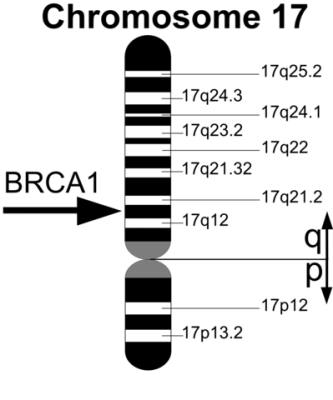
OFFICIAL MEDICAL ADVICE ON THE BRCA GENES AND BREAST CANCER. Jolie decided on the drastic surgery because her family history, and her mutant BRCA1 gene, upped her statistical risk of breast cancer to, she says, 87%. Doc Preeti Malani's Q&A with doc Boris Pasche appeared at news@JAMA. Pasche said flatly that women with no personal or family history of these cancers "should not be offered [genetic] testing."
He walks readers through genetic counseling, management options that include intensive monitoring as an alternative to surgical breast removal, and what to do with ambiguous genetic test results. "It is preferable that BRCA testing be ordered by clinicians with expertise in cancer genetics," Pasche says, adding that he expects no big increase in genetic testing as a result of Jolie's announcement.
I regard these comments as conventional medical advice, as close to the official word as we're going to get. In Pasche's scenario, the experts are firmly in charge and the patient is a vessel into which they pour their wisdom. Surprisingly old-fashioned, really.
At the Health Care Blog, Doc Shirie Leng thinks Jolie probably did the right thing given her history. But she reminds us, in some detail, that a double mastectomy is pretty horrible. Jolie seems to have been fortunate in her recovery, but for many women the surgery and its aftermath are the very definition of not fun.
It sounds as if that's what happened to Rebecca Hull, whose BRCA1 mutation prompted her double mastectomy too. Hull works for Cancer Research UK, and her blog post on the organization's site recounts a series of surgical journeys that haven't gone exactly as planned. And it's not over yet. She must still figure out whether surgery is the answer for her high risk of ovarian cancer. (Jolie must make the same decision.) Despite the rocky course of her treatment, Hull says she has no regrets.
WE PAUSE FOR A STRICTLY SCIENTIFIC INTERLUDE. A Zimmer primer on the BRCA genes at The Loom explains that the normal version of BRCA1 prevents cancer by preventing mutations in other genes and repairing broken genes. The peculiar good news about the mutant BRCA1 genes that cause breast and ovarian cancer is that women who have them tend to have more children than women with the normal BRCA1 gene. This has some intriguing evolutionary implications — which, of course, he explains.
THE TREND TO PREVENTIVE MASTECTOMY. Doc Pasche pooh-poohs the idea that the Jolie news will cause prophylactic mastectomies to increase, but apparently he hasn't looked at the trends. Nancy Shute has, and at Shots explains that a great many women who have their breasts removed because of one cancer believe they are at particular risk for recurrence. Mostly they aren't.
Shute says the rise in preventive mastectomy is an American trend not found in Europe, and today insurers generally cover the surgery and post-op reconstruction too. According to Otis W. Brawley, chief medical officer of the American Cancer Society, Obamacare will require insurers to cover counseling and testing for breast cancer risk — but not the surgery itself. Can that be true? Surely most of them will cover breast cancer surgery. Won't they?
At Maclean's Science-ish, Julia Belluz looks at the data and points out that while double mastectomy does save lives, it appears that there is no documented benefit for the majority of surgical patients with genetic risk factors. They might have lived long lives even if they had kept their breasts.
THE COST OF THE MYRIAD GENETICS PATENTS ON BRCA1 AND BRCA2 In the US, a genetic test for a cancer-causing mutant BRCA1 gene is said to cost between $3,000 and $4,000. Apparently insurance will often pay, and of course Angelina Jolie probably doesn't have to worry about her medical bills whether she has insurance or not. But what if you don't have either insurance or a hefty income? If you can wait a few months, Obamacare to the rescue; see above.
The reason the test is so expensive is that Myriad Genetics has patented BRCA1 and BRCA2, mutants and all. That seems batty to a lot of us, the idea that genes possessed by everyone on this planet can be owned by a commercial organization. Sometime in the next few weeks the US Supreme Court will let us know whether it seems batty to them, too. This being a court with much affection for commercial interests, I wouldn't bet on it. Others are not so sure, as I recounted here in April.
As a result of the Jolie mastectomies, the Myriad case has resurfaced. Andrew Cohen summarizes the back-and-forth history of the myriad Myriad court cases at The Atlantic. At Gene Expression, Razib Khan is intrigued by the fact that geneticists all seem to oppose the Myriad patents. At Patent Docs, Kevin Noonan analyzes a Nature Biotechnology article describing the history of DNA patents and arguing that the Myriad case is an anachronism because the future of biotech does not rest on patenting.
 and after. Credit: Otto J. Placik")
AND THIS JUST IN: ARE BOOB JOBS FOR BOOBS? At Journal Watch, Andrew Kaunitz describes a big BMJ study showing that breast implants increase a woman's chances of dying of breast cancer. In the US, he says, more than 300,000 women undergo breast augmentation every year.
Good grief.
